The Deep Squeeze Financial Design Killing Health Access
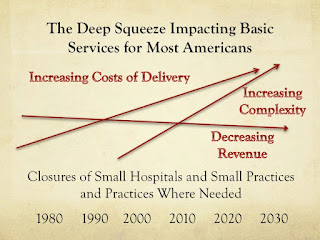
As an academic family physician specializing in basic health access, I worked to resolve shortages and improve access to care. It was my privilege to work in some of the few remaining schools devoted to such efforts. Sadly this professor found that he was learning impaired - or perhaps I was indoctrinated by the process of medical education. The financial design was far too powerful to allow training design to address deficits. What appeared to work in the 1965 to 1980 period of time, worked because of the financial design. Each year more dollars were pumped into basic services - especially where poor Americans and seniors were found. As it turns out, these are the areas with the most deficits. Initially the original Medicare and Medicaid designs helped, but they were changed into vehicles to concentrate dollars - not distribute care. The same designers continue to shape the designs into more for few and fewer for more - and basic health access suffers most by design. My solo rural...


